I feel women have made a lot of progress on un-tabooing several issues that we as a gender have had to deal with for ages mostly in silence, because society in general has pressured everyone into keeping these private (or among girlfriends): girls getting their first period (menarche), pregnancy and labor (the British show “call the midwife” does a great job at presenting several women issues as they were dealt with in the 1950s and 60s), contraception, post-partum depression, premenstrual syndrome (PMS), female genital mutilation, etc. Even menopause, although more recognized and talked about now, has been sort of “simplified”, generally omitting the period known as “perimenopause” which precedes the actual menopause and can be, for many women, a loooong process characterized by more than a few different (and annoying) symptoms. As with PMS, even among medical professionals this “condition” is not widely recognized, and hence often misdiagnosed and not dealt with in a helpful manner.
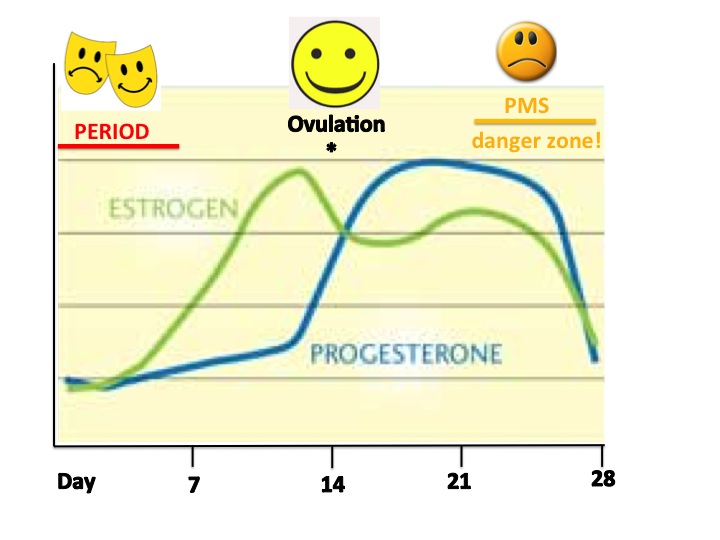
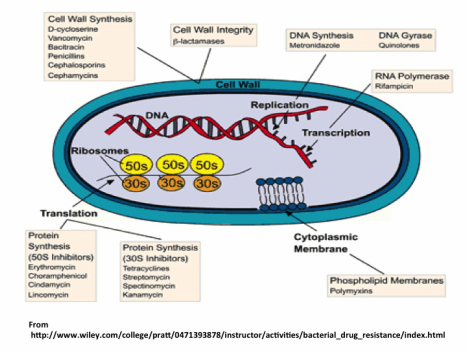
Some women have it easy both for PMS as well as for the rollercoaster that perimenopause can be, physically and emotionally. For those of us not so lucky, knowing the causes may bring some AHA moments and perhaps better ways to deal with the symptoms. In both cases, symptoms experienced are mainly due to hormone levels fluctuating. The main hormones are estrogen and progesterone (both produced in the ovaries; estrogen is produced in response to other hormones (FSH and LH) that stimulate the ovaries to do so, produced by the pituitary gland in the brain), which go up and down periodically in a monthly (lunar) fashion to result in our menstrual cycles or periods, as shown in the figure. Progesterone, produced in the ovary after ovulation, starts preparing the uterus for a fertilized egg, making it thicker with increased blood supply. If fertilization or implantation do not occur, the egg disintegrates and levels of estrogen and progesterone drop and the uterus contracts and period (bleeding) comes. It is the sudden drop in progesterone that occurs right before we bleed which causes many PMS symptoms.
Some women have it easy both for PMS as well as for the rollercoaster that perimenopause can be, physically and emotionally. For those of us not so lucky, knowing the causes may bring some AHA moments and perhaps better ways to deal with the symptoms. In both cases, symptoms experienced are mainly due to hormone levels fluctuating. The main hormones are estrogen and progesterone (both produced in the ovaries; estrogen is produced in response to other hormones (FSH and LH) that stimulate the ovaries to do so, produced by the pituitary gland in the brain), which go up and down periodically in a monthly (lunar) fashion to result in our menstrual cycles or periods, as shown in the figure. Progesterone, produced in the ovary after ovulation, starts preparing the uterus for a fertilized egg, making it thicker with increased blood supply. If fertilization or implantation do not occur, the egg disintegrates and levels of estrogen and progesterone drop and the uterus contracts and period (bleeding) comes. It is the sudden drop in progesterone that occurs right before we bleed which causes many PMS symptoms.
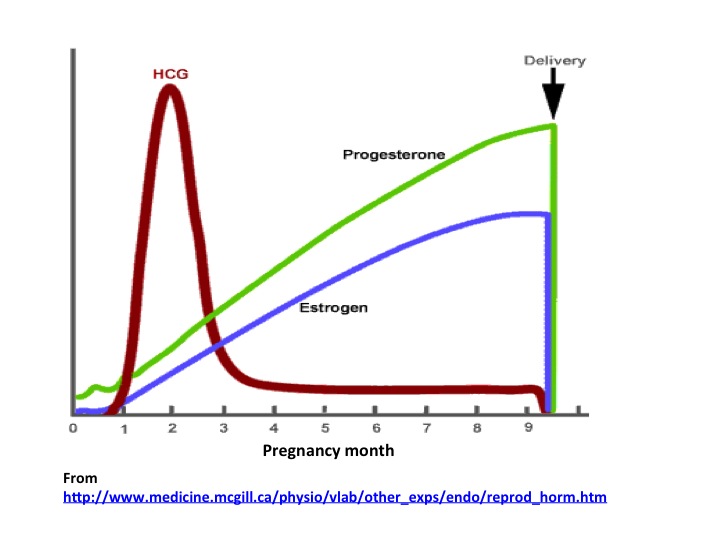
An even more drastic drop in progesterone levels occurs after delivering a baby- before pregnancy, women produce about 20 mg of progesterone daily; this level goes up to 400 mg a day during pregnancy, and this drops abruptly right after delivery (the placenta is very rich in progesterone). After delivery, and until the woman starts menstruating again (usually inhibited during breastfeeding) levels of progesterone (as well as estrogen) are super low, and this may have a lot to do with post-partum depression.
Testosterone, although considered a predominantly male hormone, is also produced in low amounts by women, with roles in promoting muscle building and muscle tone, increase libido, and strengthening bones. As do estrogen and progesterone, also testosterone levels decline in older women.
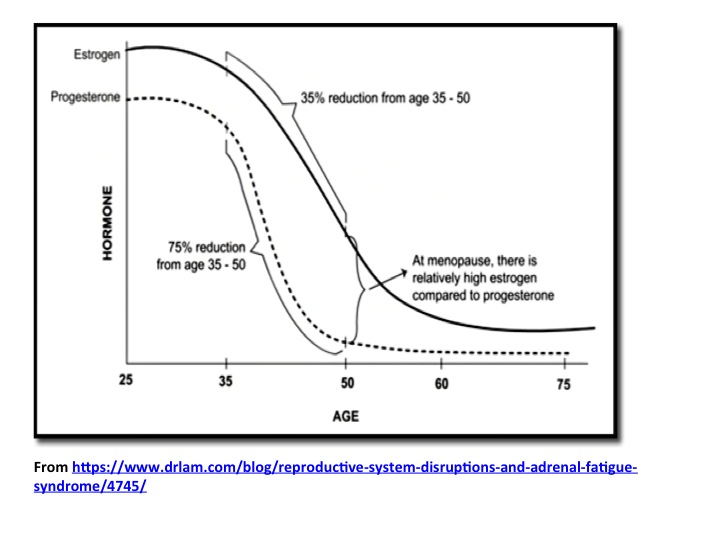
Perimenopause can start as early as late 30s or early 40s, while menopause (defined as 12 months or more without periods) occurs in average when women are around 51-52 years old. So if you do the math, perimenopause in some women can last up to 10 years, while others do not experience any major symptoms or they do for a much shorter time. The average time is 3-4 years. This "condition" is a transition due to hormone levels, although in this case is rather due to proportional levels of estrogen and progesterone (one compared to the other). A condition known as estrogen dominance, in which the drop in estrogen is small compared to the drop in progesterone, usually occurs in perimenopause and as a result there is a relative increase of estrogen in the body when compared to progesterone levels, all while the levels of these two hormones are generally declining during the years preceding menopause. Because of this estrogen dominance, this is a good time to be aware of xenoestrogens we are increasingly exposed to nowadays (for more on this see my post on endocrine disruptors).
Perimenopause can start as early as late 30s or early 40s, while menopause (defined as 12 months or more without periods) occurs in average when women are around 51-52 years old. So if you do the math, perimenopause in some women can last up to 10 years, while others do not experience any major symptoms or they do for a much shorter time. The average time is 3-4 years. This "condition" is a transition due to hormone levels, although in this case is rather due to proportional levels of estrogen and progesterone (one compared to the other). A condition known as estrogen dominance, in which the drop in estrogen is small compared to the drop in progesterone, usually occurs in perimenopause and as a result there is a relative increase of estrogen in the body when compared to progesterone levels, all while the levels of these two hormones are generally declining during the years preceding menopause. Because of this estrogen dominance, this is a good time to be aware of xenoestrogens we are increasingly exposed to nowadays (for more on this see my post on endocrine disruptors).
The most commonly reported symptoms by women in perimenopause are changes in menstrual cycle (shorter or longer, lighter or heavier, etc), followed by a myriad of others which may or may not be present in different combinations in different women: hot flashes and night sweats, insomnia, strong headaches or migraines around the time of the menses, exhaustion, lethargy, clumsiness, new or stronger conditions (such as allergies), worse lower back ache with menses, dry and itchy skin, food cravings and digestive disturbances including constipation and diarrhea, dark circles around the eyes, hair loss/thinning (and unusual hair growth in other places), breast swelling and soreness before bleeding, loss of libido and vaginal dryness, dizziness, tinnitus (ringing in the ears), quick weight gain especially on the waist, buttocks and thighs, fluid retention, palpitations, change in body odor, depression, etc etc etc….
Depending on your own experience, whom you ask or what site you read, the list of symptoms of peri menopause can be very VERY long.
Because estrogen is also an important factor in maintaining women's bone and cardiovascular health, women undergoing early or premature menopause (menopause before the age of 40, which can occur naturally or induced due to medical treatments such as chemotherapy or radiation for cancer) are usually recommended to take HRT (hormone replacement therapy) for a few years to prevent bone loss and osteoporosis. HRT may help ease other symptoms like hot flashes, night sweats, and vaginal dryness, and mood swings. However, HRT use is controversial as it may increase the risk of cancer, stroke, and blood clots. It is also contraindicated if there is a history of breast or endometrial cancer, liver disease, blood clots, or stroke. If symptoms are not as bad as to make you consider taking hormones, then getting good rest, healthy eating (avoiding stimulants and alcohol may help) and getting regular exercise and relaxation activities can go a long way into helping you deal with hormonally imposed havoc.
The age at which a woman will reach menopause, as well as the probability to go through menopause prematurely are known to have a strong genetic component, so find out when your mother did and you will have an idea of what to expect.
The age at which a woman will reach menopause, as well as the probability to go through menopause prematurely are known to have a strong genetic component, so find out when your mother did and you will have an idea of what to expect.


 RSS Feed
RSS Feed