I wrote about COVID-19 and coronaviruses when the pandemic first started spreading worldwide in March 2020. There have been now roughly 100 million cases and a bit over 2 million deaths due to this disease, with the USA one of the main contributors.
In an unprecedented effort to face the pandemic and in addition to national, regional and global initiatives in terms of implementing safety measures such as lockdowns including school and stores closures, mask wearing, PPE and testing, etc, we count now with an impressive number of vaccines approved as well as at different stages of development and in clinical trials. More types of vaccines are being developed simultaneously for COVID-19 than for any other infectious disease before.
In an unprecedented effort to face the pandemic and in addition to national, regional and global initiatives in terms of implementing safety measures such as lockdowns including school and stores closures, mask wearing, PPE and testing, etc, we count now with an impressive number of vaccines approved as well as at different stages of development and in clinical trials. More types of vaccines are being developed simultaneously for COVID-19 than for any other infectious disease before.
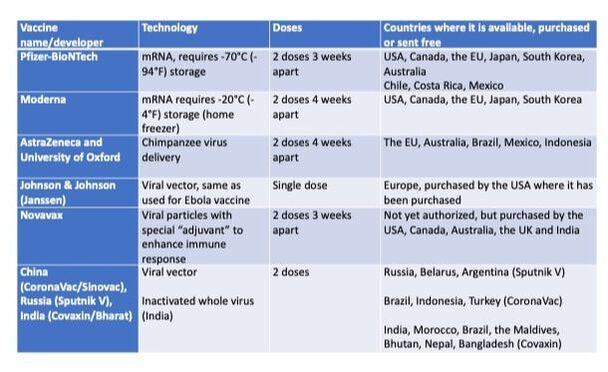
Although usually the FDA approval process is long (it can take years), emergency authorization is now given to COVID-19 vaccines with less data than otherwise required but based on enough evidence that they are safe and effective. The first two COVID-19 vaccines very recently approved in the USA for emergency use are based on a new (mRNA) vaccine technology, making them the first of this type to be approved for use in humans: the Pfizer-BioNTech and Moderna vaccines got 2020 FDA approval on December 11 and 19, respectively. These two vaccines have been manufactured and distributed to different countries, mostly high-income, as they require storing at very cold (freezer) temperatures to keep the very labile mRNA from degrading and are the most expensive per dose. The USA, Canada, many European countries and Japan have purchased many doses of one or both of these vaccines for their populations, and Mexico, Chile and Costa Rica in Latin America have also started Pfizer vaccination in December 2020. Regions and countries started preordering vaccines (in millions of doses) when candidate vaccines showed promising results in clinical trials.
All other vaccines approved to date can be stored at fridge temperatures. These vaccines use different technologies that don’t involve RNA, for example viral vectors are used that have been engineered to carry information on the antigen from the virus, which for COVID-19 is the Spike protein, and to not be able to replicate in human cells. One such vaccine was developed by AstraZeneca and University of Oxford, it got approved by the UK on December 30, 2020. The first registered vaccine was the Russian Sputnik V, in August 2020 before phase 3 clinical trials started, which has been used in Argentina since December 2020. The Janssen (Johnson & Johnson) vaccine is expected to get FDA emergency use approval soon in the USA, the third one after Pfizer and Moderna. This vaccine is the only one so far offering a single dose regimen instead of two.
All other vaccines approved to date can be stored at fridge temperatures. These vaccines use different technologies that don’t involve RNA, for example viral vectors are used that have been engineered to carry information on the antigen from the virus, which for COVID-19 is the Spike protein, and to not be able to replicate in human cells. One such vaccine was developed by AstraZeneca and University of Oxford, it got approved by the UK on December 30, 2020. The first registered vaccine was the Russian Sputnik V, in August 2020 before phase 3 clinical trials started, which has been used in Argentina since December 2020. The Janssen (Johnson & Johnson) vaccine is expected to get FDA emergency use approval soon in the USA, the third one after Pfizer and Moderna. This vaccine is the only one so far offering a single dose regimen instead of two.
All COVID-19 vaccines so far are designed to get our immune system to develop a strong response to the virus by delivering the Spike protein that covers the surface of the virus (acting as an “antigen” against which we will make antibodies) or parts of it. All approved vaccines, even for emergency use, have shown considerable protection in clinical trials, meaning a much lower risk of getting COVID-19 for vaccinated versus non-vaccinated people. As more people get vaccinated, more data on different vaccines will be available. In the USA, depending on where people live, they are currently getting either the Pfizer or the Moderna vaccine.

The process of approving vaccines, rollout protocols and guidelines for use all vary considerably between regions and countries. Some countries, including Japan, South Korea, Brazil and India have deals in place to manufacture themselves some of the available vaccine formulations. As more vaccines are approved, distributed and available, people wonder if some are better than others and whether they could choose one or wait for a different one not yet available. The recommendation is to get whichever is available in your area- it will protect you if it has been approved for use. If shortages occur for some vaccines or authorities decide to use the existing supply to give the first dose to more people without necessarily saving enough shots for the second dose, giving a second dose of a different available vaccine is considered, or allowing a longer time gap between doses until more vaccine shots are available.
Because clinical trials are first conducted in adults, COVID-19 vaccines are not yet approved for use in under 16-18 year old children, but trials in younger children are currently underway and a vaccine may become available either by the end of 2021 or in 2022.
Because clinical trials are first conducted in adults, COVID-19 vaccines are not yet approved for use in under 16-18 year old children, but trials in younger children are currently underway and a vaccine may become available either by the end of 2021 or in 2022.

This week, the USA joined COVAX, a global initiative that includes WHO, UNICEF, Gavi (the Vaccine Alliance) and CEPI (the Coalition for Epidemic Preparedness Innovations) to ensure rapid and equitable access to COVID-19 vaccines for all countries, aiming to cover at least 20% of each participating population by the end of 2021 by providing two billion vaccines this year. Some vaccine manufacturers have pledged a considerable number of doses to low income countries.


 RSS Feed
RSS Feed