In a previous post on immunotherapy I touched briefly upon the immune system, whose function is to keep us free of dangerous pathogens including viruses, bacteria and parasites. The basic principle is that specialized cells produce “antibodies” which recognize the invading foreign “antigen” (molecules present usually on the surface of the threat organism) and after binding to them, a complex and specialized response is activated that involves different types of molecules and cells (depending on the pathogen) to result in destruction of the pathogen.
There is also “memory” in these antibody-producing cells that triggers an even more potent response when the same antigen infects us for the second time. This is the mechanism by which vaccines provide protection. The first response we get to the “immunizing” vaccine, which is usually a dead virus/bacteria or a purified/synthetic antigen (part) of the organism that produces the disease, is of low intensity. If/when our bodies are exposed to the real thing (the live pathogen) later on, the immune system activates the old cells that “saw” the vaccine antigen and a strong immune response keeps the infection under control. This immunization can be life-long for some vaccines, or last several years after which re-vaccination is recommended.
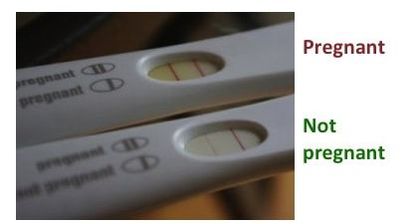
Many tests used by clinicians, laboratories or by us at home (pregnancy test or EPT) are based on the antigen-antibody interaction that occurs once the antibody recognizes its particular antigen. In the test device there is an antibody present (as well as other reagents necessary for the interaction to happen) which will recognize the antigen of an organism or cell we are evaluating. We need to provide a “sample” (usually blood, or urine for EPT, or in some cases saliva) that contains this antigen if we are “infected” or “positive” for the condition measured. Given some time for the antigen-antibody reaction to occur after the liquid sample is allowed to contact the reagents in the test, there will be some indication (color, a line) if we are “positive”. Just to make sure that all the things in the device are working well, a “positive control” is usually included, which will be a positive band indicating the test works well. The reading is read as “positive” or “negative” in medical terms. In the EPT photo below, the line on the right present in both positive (top test) and negative (bottom test) results is the positive control.
Many tests used by clinicians, laboratories or by us at home (pregnancy test or EPT) are based on the antigen-antibody interaction that occurs once the antibody recognizes its particular antigen. In the test device there is an antibody present (as well as other reagents necessary for the interaction to happen) which will recognize the antigen of an organism or cell we are evaluating. We need to provide a “sample” (usually blood, or urine for EPT, or in some cases saliva) that contains this antigen if we are “infected” or “positive” for the condition measured. Given some time for the antigen-antibody reaction to occur after the liquid sample is allowed to contact the reagents in the test, there will be some indication (color, a line) if we are “positive”. Just to make sure that all the things in the device are working well, a “positive control” is usually included, which will be a positive band indicating the test works well. The reading is read as “positive” or “negative” in medical terms. In the EPT photo below, the line on the right present in both positive (top test) and negative (bottom test) results is the positive control.
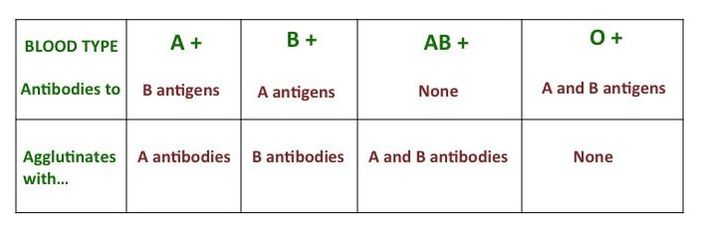
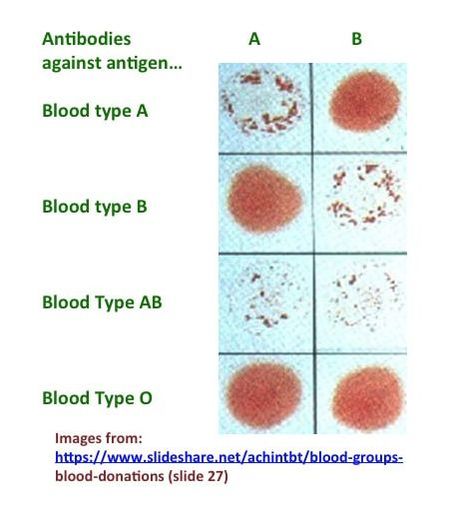
The best example of an antigen-antibody test is the blood type test based on “agglutination” (for background on blood types see my previous post on this subject). Given a sample of your blood, it will agglutinate (clump) when it “sees” the right antibody: blood type A which contains type A antigens on the surface of red cells will agglutinate with anti-A antibodies; blood type B with anti-B antibodies. You can “read” your blood type as shown in the figure below, by exposing it to anti-A and anti-B antibodies separately in a blood type agglutination test: blood type O will not agglutinate with either antibody, whereas blood type AB will do with each antibody. Anti-Rh antibodies are also used in the assay to determine whether you are Rh + or – (not shown in the table or picture below- see my post on blood types for details on Rh factor). I remember doing this in an immunology laboratory course in Caracas, Venezuela as part of my undergraduate “licenciatura” in cell biology. We had a lab session dedicated to this topic, each of us used finger prick blood and tested it as shown in the picture (also including an anti-Rh antibody spot) - everybody learned or confirmed their blood types; we had all of 4 blood groups represented in our class.
Other rapid tests that can be performed quickly with blood samples even in rural settings where laboratory settings/hospitals/clinics are not at reach are malaria and HIV tests. The HIV test however, although continuously evolving into a more “sensitive” one, may not detect antibodies in an infected person during the so called “window” period up to 3 months in which the infected person is contagious to others. A more definitive test for any condition, which detects the presence of the antigen specifically, is one based on molecular tools such as PCR. But these tools requires specialized equipment and reagents, sample processing and storage, and are more expensive.

 RSS Feed
RSS Feed