Antibiotics are antimicrobial substances produced by various species of microorganisms (bacteria, fungi) that suppress the growth of other microorganisms. Nowadays, antibiotics also include synthetic or semi-synthetic agents not produced by microbes, such as sulfonamides and metronidazole. Thanks to the discovery and subsequent medical use of antibiotics in the early 1900s, many bacterial infections that used to be lethal or cause high morbidity are now a thing of the past. The modern era of antimicrobial therapy started with the clinical use of sulfonamide in 1936, followed by production of penicillin in 1941. Penicillin was so successful in treating bacterial infections that the search for other antibiotics was slowed down.
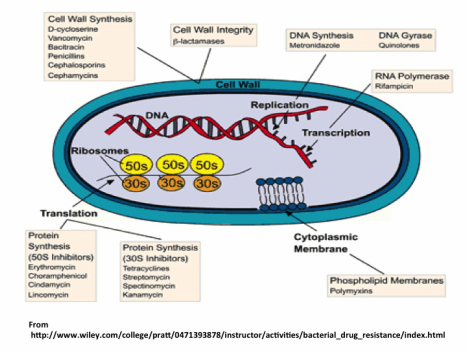
The way antibiotics work is by altering or inhibiting bacterial cell structures or processes that are essential for bacterial growth. These mechanisms and specific antibiotics for each are shown in the figure below showing a cell and its parts. The most common mechanism of action is by inhibiting the making of the cell wall (penicillins and cephalosporins) by targeting its major structural component, the peptidoglycan layer. Other antibiotics affect the structure of the cellular membrane, whereas some act by inhibiting protein synthesis (tetracyclines, macrolides and clindamycin), synthesis of DNA or RNA (metronidazole and quinolones, rifampicin) or a metabolic pathway (sulfonamides). Antibiotics that kill bacteria (bactericidal) include the penicillin group that kills susceptible bacteria by inhibiting the synthesis of the bacterial peptidoglycan cell wall that provides the cell with rigidity.
The way antibiotics work is by altering or inhibiting bacterial cell structures or processes that are essential for bacterial growth. These mechanisms and specific antibiotics for each are shown in the figure below showing a cell and its parts. The most common mechanism of action is by inhibiting the making of the cell wall (penicillins and cephalosporins) by targeting its major structural component, the peptidoglycan layer. Other antibiotics affect the structure of the cellular membrane, whereas some act by inhibiting protein synthesis (tetracyclines, macrolides and clindamycin), synthesis of DNA or RNA (metronidazole and quinolones, rifampicin) or a metabolic pathway (sulfonamides). Antibiotics that kill bacteria (bactericidal) include the penicillin group that kills susceptible bacteria by inhibiting the synthesis of the bacterial peptidoglycan cell wall that provides the cell with rigidity.
Because antibiotics target specific processes and structures in bacteria, they do not affect our cells and are supposedly “safe” to take. However, although antibiotics do not kill human cells, they do end up killing some of the “good” bacteria that make our resident microbiomes (see my post on microbiomes for more info). Taking too much or too many rounds of antibiotics (sometimes unnecessary, such as when wrongly or self-prescribed) within a certain time makes it hard for these communities of good bacteria to regrow inside us.
Unfortunately, prescribing antibiotics is common practice in many countries even before evidence of a bacterial infection in the patient is available. In fact, antibiotics are the most overprescribed drugs. They work as anti-bacterial (also against fungi and parasites) agents but not for viral infections, such as colds or the flu. For some viral infections such as influenza, herpes, and HIV the drugs taken are called antivirals. A current public health problem is the emergence and spread of drug-resistant infections (check my previous post on this subject if you are interested).
Unfortunately, prescribing antibiotics is common practice in many countries even before evidence of a bacterial infection in the patient is available. In fact, antibiotics are the most overprescribed drugs. They work as anti-bacterial (also against fungi and parasites) agents but not for viral infections, such as colds or the flu. For some viral infections such as influenza, herpes, and HIV the drugs taken are called antivirals. A current public health problem is the emergence and spread of drug-resistant infections (check my previous post on this subject if you are interested).

In 2014, the World Health Organization (WHO) issued the first report on antimicrobial resistance, including antibiotic resistance, defined as when bacteria change so antibiotics no longer work in people who need them to treat infections, now a major threat to public health. Just this week the first “super bug” was found in the US in a woman infected with a strain of E. coli (a common intestinal bacteria in humans and other animals) resistant to many antibiotics, including those used as a last resort when infections are found to be drug resistant.
Bacteria in food can also become resistant because of the use of antibiotics in animals. These resistant bacteria can contaminate meat and other animal products, as well as the environment when animal waste products spread to produce via contaminated water used for irrigation.
Bacteria in food can also become resistant because of the use of antibiotics in animals. These resistant bacteria can contaminate meat and other animal products, as well as the environment when animal waste products spread to produce via contaminated water used for irrigation.
Because antibiotics act very quickly to kill MOST bacteria that cause infection (in about 24-48h) many people taking them are tempted to stop earlier than the prescribed full course (a week or 10 days sometimes). However, there will be remaining bacteria, and among these, the ones “selected” by the antibiotic and resistant to it will be enriched and will survive and reproduce. In low resources settings, it is common to save the leftover antibiotics and take them later on if the infection comes back, risking treatment failure due to expired or damaged antibiotics, as well as emergence and spread of drug resistance.

 RSS Feed
RSS Feed